
Behavioral Health Onboarding Program
Designing a performance-driven learning experience to improve compliance, confidence, and early-stage retention.
Overview
The Audience
Newly hired Behavioral Health Technicians (0–12 months of experience)
Responsibilities
Instructional Design
Interactive eLearning Development
Visual Learning Design
Scenario-Based Experience Design
Tools Used
Articulate Rise
Storyline 360
Canva
Adobe Premiere
The Problem
Behavioral health organizations often experience high turnover within the first 90 days of employment, particularly among newly hired Behavioral Health Technicians (0–12 months of experience). Early-stage attrition is frequently driven by unclear role expectations, inconsistent onboarding processes, compliance-related anxiety, and limited confidence in documentation and professional boundaries. New hires enter high-accountability, client-facing environments where mistakes can carry regulatory and ethical consequences. Without structured, applied onboarding, technicians may feel overwhelmed navigating HIPAA requirements, documentation standards, and real-world boundary decisions. This gap between training and applied performance increases compliance risk, slows competency development, and negatively impacts retention and service quality.
Projected risk indicators included:
Documentation error rates within the first 60 days
Lower first-attempt compliance assessment scores
Reduced 90-day retention
Low self-reported confidence in boundary and documentation procedures

The Solution
Behavioral health organizations often experience high turnover within the first 90 days of employment, particularly among newly hired Behavioral Health Technicians (0–12 months of experience). Early-stage attrition is frequently driven by unclear role expectations, inconsistent onboarding processes, compliance-related anxiety, and limited confidence in documentation and professional boundaries. New hires enter high-accountability, client-facing environments where mistakes can carry regulatory and ethical consequences. Without structured, applied onboarding, technicians may feel overwhelmed navigating HIPAA requirements, documentation standards, and real-world boundary decisions. This gap between training and applied performance increases compliance risk, slows competency development, and negatively impacts retention and service quality.
Projected risk indicators included:
Documentation error rates within the first 60 days
Lower first-attempt compliance assessment scores
Reduced 90-day retention
Low self-reported confidence in boundary and documentation procedures
Creating the Process
I used the ADDIE model as a foundational framework, layered with scenario-based and adult learning principles.
During the analysis phase, I identified a performance issue impacting early-stage retention and compliance among newly hired Behavioral Health Technicians (0–12 months of experience). Behavioral health organizations were experiencing elevated turnover within the first 90 days, driven by unclear role expectations, inconsistent onboarding processes, compliance-related anxiety (including HIPAA and documentation standards), and low confidence in navigating professional boundaries. There was a clear gap between theoretical onboarding content and applied, client-facing performance expectations. These gaps created measurable business risks, including increased documentation error rates within the first 60 days, lower first-attempt compliance assessment scores, reduced 90-day retention, and slower competency development. To better define the problem, I conducted a needs and risk analysis by reviewing existing onboarding materials, examining documentation error trends, identifying high-risk compliance decision points, and defining measurable performance objectives aligned with regulatory and ethical standards.
Analysis
During the design phase, I developed a structured onboarding strategy centered on applied performance rather than passive policy review. Learning objectives were written as measurable, behavior-based outcomes focused on accurate documentation, HIPAA-aligned decision-making, and professional boundary navigation in client-facing environments. I mapped high-risk compliance scenarios and structured the learning experience to include modeling, guided practice, and independent application. Scenario-based simulations and decision-making exercises were intentionally embedded to mirror real workplace challenges. Assessment strategies were designed to evaluate applied competence rather than content recall, ensuring alignment between training activities and on-the-job expectations.
Design
During the design phase, I developed a structured onboarding strategy centered on applied performance rather than passive policy review. Learning objectives were written as measurable, behavior-based outcomes focused on accurate documentation, HIPAA-aligned decision-making, and professional boundary navigation in client-facing environments. I mapped high-risk compliance scenarios and structured the learning experience to include modeling, guided practice, and independent application. Scenario-based simulations and decision-making exercises were intentionally embedded to mirror real workplace challenges. Assessment strategies were designed to evaluate applied competence rather than content recall, ensuring alignment between training activities and on-the-job expectations.
Development
The onboarding solution was integrated into the first 30 days of employment through a blended delivery approach combining facilitated discussion and scenario-based training modules. New hires engaged in applied simulations prior to independent client documentation, allowing them to practice decision-making in a lower-risk environment. Supervisors were equipped with structured observation tools and feedback checklists to reinforce skill application during early client interactions. This approach emphasized performance transfer, ensuring that learning extended beyond training completion into real-world behavioral execution.
Implementation
To evaluate effectiveness, I aligned training outcomes with measurable performance and retention indicators. Evaluation metrics included documentation accuracy rates within the first 60 days, first-attempt compliance assessment performance, supervisor-rated procedural fidelity, and 90-day retention comparisons. Self-reported confidence surveys were also used to measure shifts in perceived preparedness for documentation and boundary decisions. This evaluation framework ensured that the onboarding redesign was assessed based on business impact, compliance risk mitigation, and workforce stability rather than course completion alone.
Evaluation
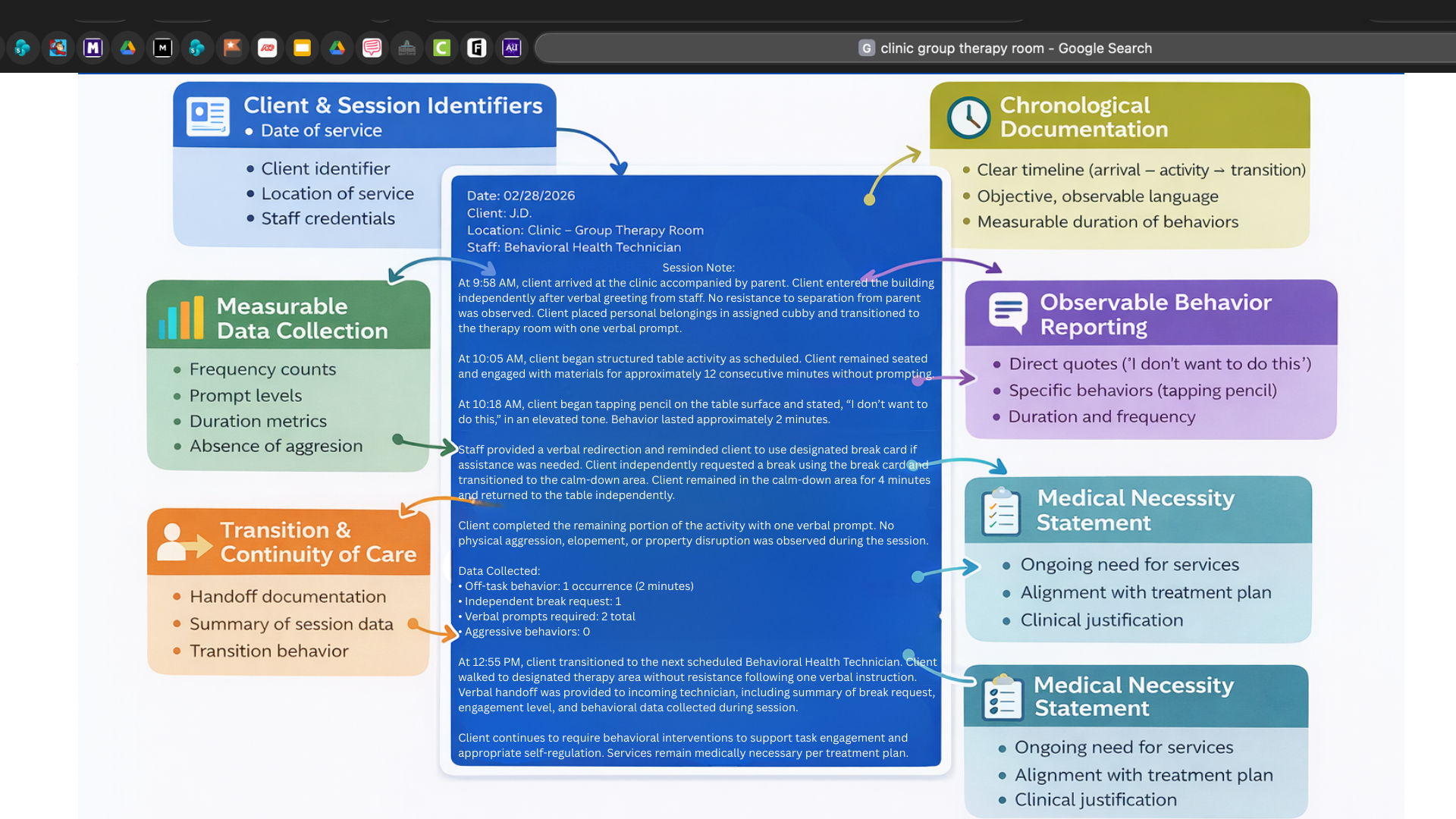
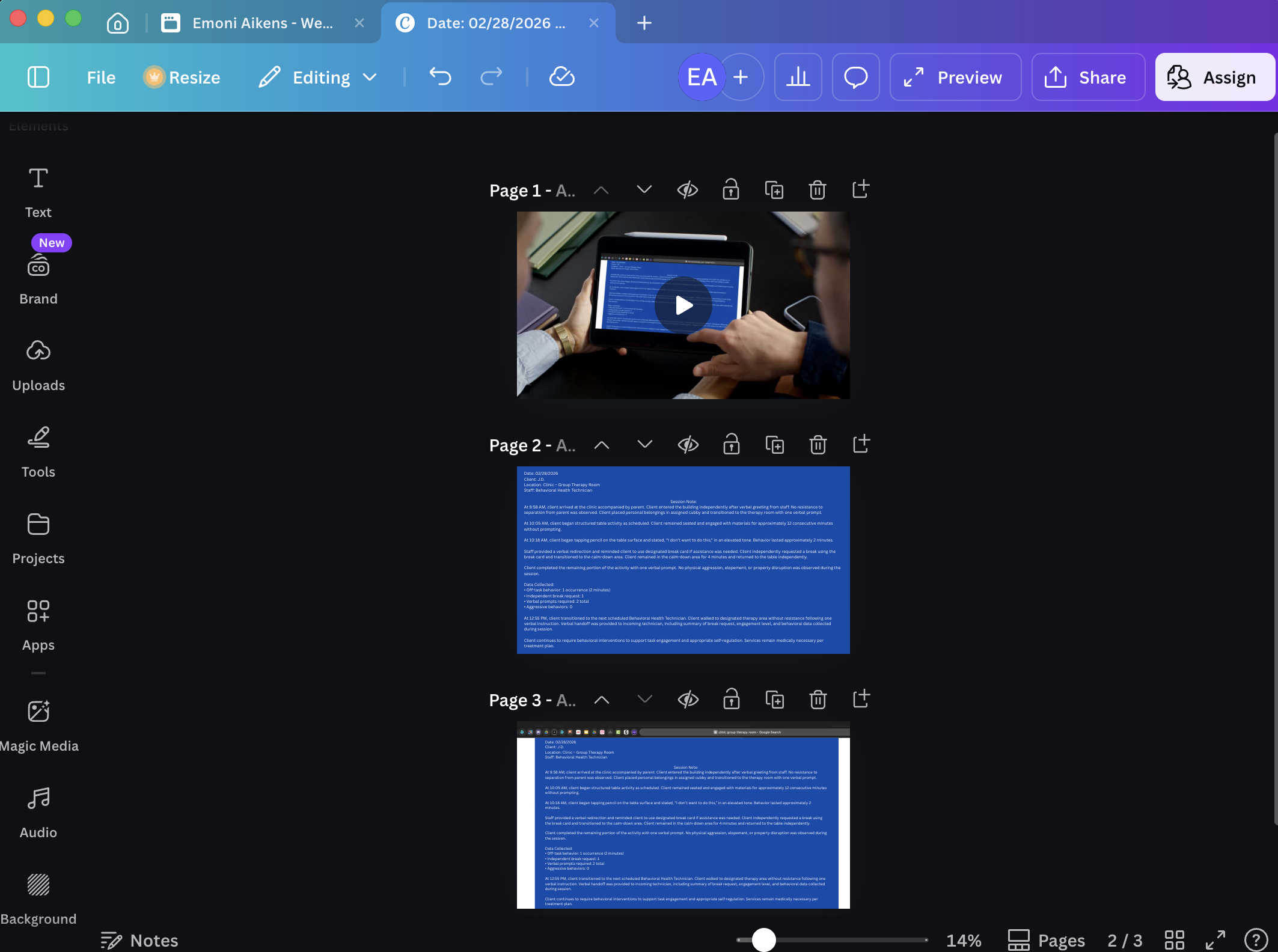
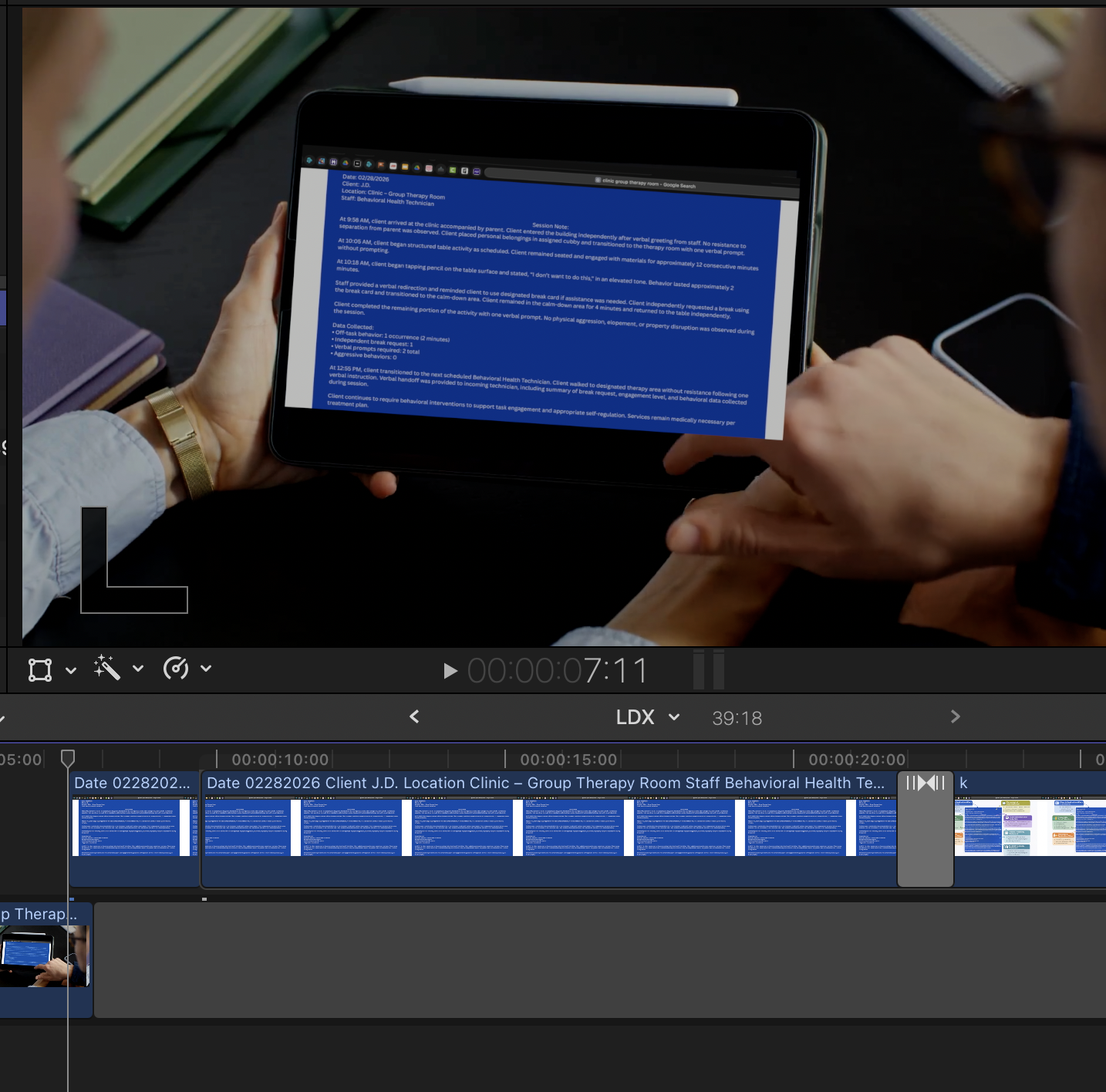
For the session note project, I first drafted a sample session note to demonstrate proper documentation structure and language. I then used Canva to design a clear visual layout that highlighted key components of effective documentation. To provide additional context, I added diagram elements that explained how each part of the session note connects to compliance and reporting expectations. Finally, I incorporated the designed content into a short instructional video and completed the final edit using Adobe Premiere, creating a visual walkthrough that models accurate session note development and documentation practices.
Design Elements

For the visual design of the instructional presentation, I chose a light grey and orange color scheme to support clarity, focus, and emotional tone. The light grey background was selected to create a neutral and professional visual environment that would not distract from the instructional content. It also helps reduce visual fatigue and allows key information to remain the central focus of each slide. Orange was used as the accent color throughout the presentation to draw attention to important elements such as headings, key terms, and decision points. From a psychological perspective, orange is often associated with energy, encouragement, and engagement. In behavioral health settings, this color can help create a sense of warmth and approachability while still maintaining a professional tone. It is frequently used to signal action and motivation, which aligns well with training focused on applied skills and behavioral decision making. By pairing orange with a neutral grey base, the design balances visual stimulation with clarity, guiding the learner’s attention while maintaining a calm and structured learning environment.
Color Schemes
I designed these scenarios to simulate realistic ethical and documentation decisions that Behavioral Health Technicians face in clinical practice. The goal is to move learners beyond memorizing policies and instead place them in situations where they must apply professional judgment. The end goal is to help learners understand that behavioral health work involves continuous ethical decision making. Through realistic dialogue and situational choices, the learner practices evaluating how documentation, boundaries, and honesty in reporting directly influence treatment quality, clinical oversight, and professional accountability. The correct response to each scenario results in instant feedback to the learner, helping them to stay encouraged and informed through the onboarding process.
Scenario Dialogue Map
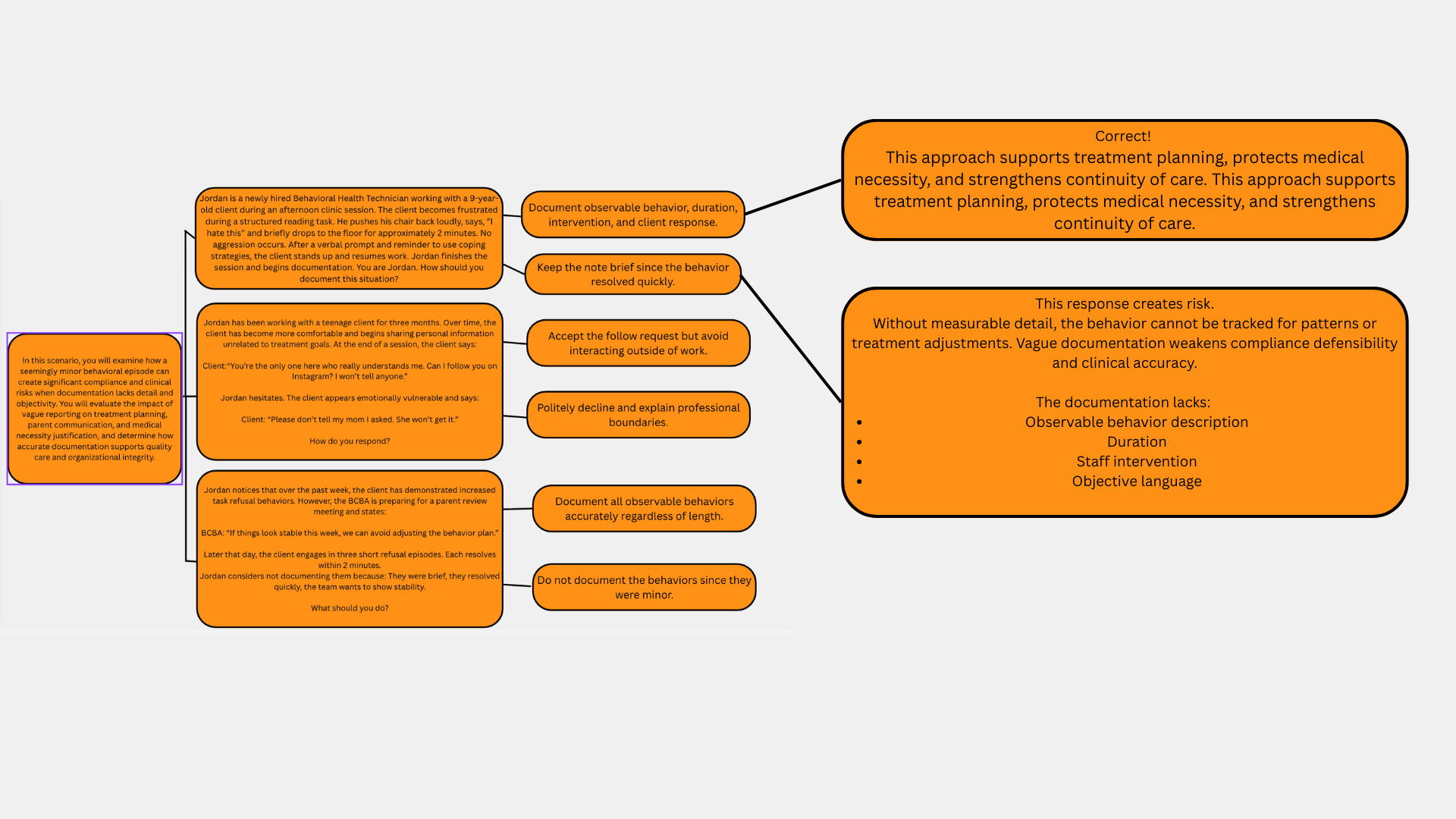
scenario 1
In the first scenario, the situation focuses on documentation accuracy. The client experiences a brief frustration episode during a structured reading task, but the behavior resolves quickly and does not escalate into aggression. The situation may appear minor, yet the scenario illustrates how even small behavioral events must be documented objectively and with clear detail. The reasoning behind including this example is to show learners that vague or incomplete reporting can affect treatment planning, parent communication, and the justification of medical necessity for services. By placing the learner in Jordan’s role, the scenario prompts them to consider what objective documentation looks like and why accurate records protect both the client and the organization. The learner must recognize that behaviors should be recorded using observable language, time references, and factual descriptions rather than personal interpretation.
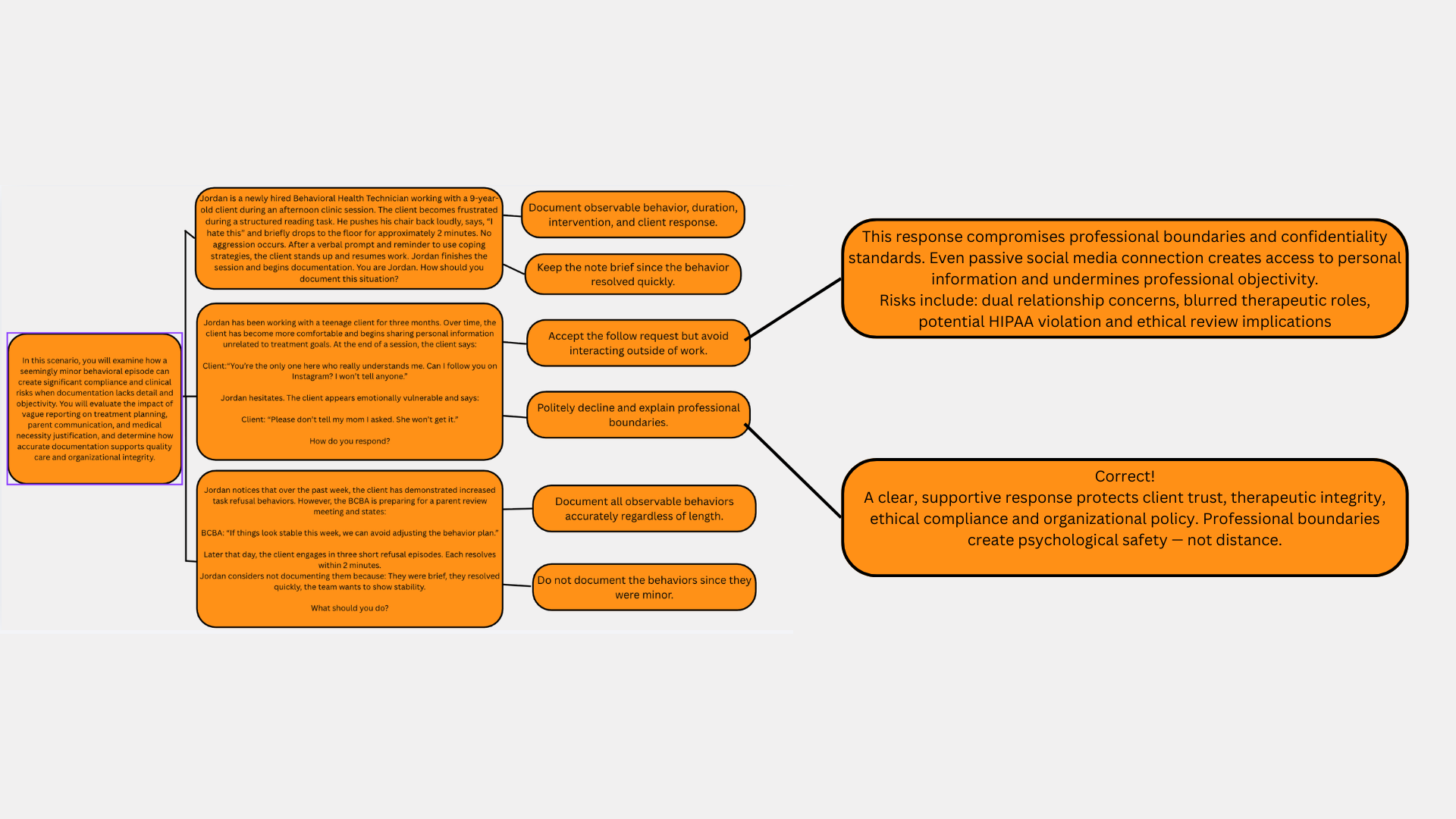
scenario 2
The second scenario addresses professional boundaries and confidentiality in therapeutic relationships. As the client becomes more comfortable, they begin requesting personal contact through social media and ask Jordan to keep the request private from their parent. This situation was likely designed to demonstrate how easily boundary lines can blur when working closely with clients who are emotionally vulnerable. The reasoning behind this dialogue is to highlight that technicians must maintain professional distance, protect confidentiality, and follow organizational policies even when a client expresses trust or emotional dependence. By presenting the learner with a direct request from the client, the scenario encourages them to practice responding in a way that is supportive but still ethically appropriate.
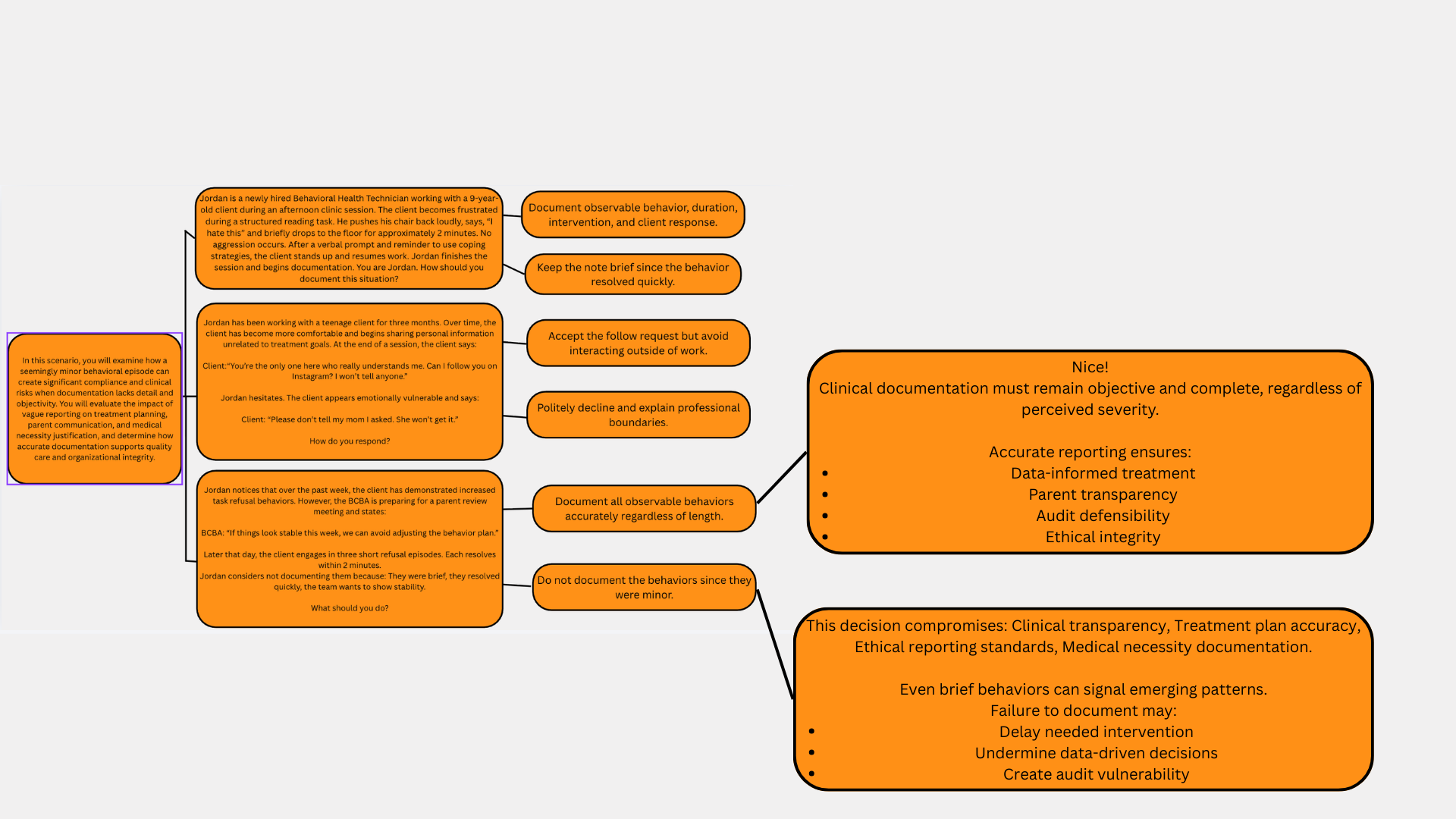
scenario 3
The third scenario focuses on ethical responsibility and data integrity. Jordan notices an increase in task refusal behaviors, but there is subtle pressure from the team to maintain the appearance of stability before a parent review meeting. The reasoning behind this scenario is to demonstrate the real-world tension between organizational expectations and ethical documentation practices. Even though the refusal behaviors are short and resolve quickly, they still represent meaningful data points. If Jordan chooses not to document them, the behavior plan could be based on inaccurate information. This scenario encourages learners to recognize that accurate data collection supports effective intervention planning and maintains transparency with families and supervising clinicians.